Key Takeaways
IBS is real, common and not “in your head,” but it is a diagnosis of exclusion: a label for a pattern of symptoms, not an explanation of their cause.
The core symptoms are recurring abdominal pain or cramping, bloating and a change in bowel habit, diarrhoea, constipation or both, now grouped into subtypes (IBS-D, IBS-C and IBS-M).
IBS is best understood as a disorder of gut-brain interaction, in which the gut bacteria, the gut lining, the immune system and the nervous system are all involved.
Common, identifiable drivers include gut dysbiosis and SIBO, intestinal permeability, food intolerances, stress and digestive insufficiency, and in some people IBS begins after a gut infection.
Functional testing (stool, breath and food-sensitivity testing) can identify which driver is present, so support is targeted rather than generic.
Some symptoms are not IBS: blood in the stool, unexplained weight loss, or new bowel changes after 50 need a GP, not guesswork.
Jump To
Bloated, Cramping and Planning Your Day Around the Loo? It Could Be IBS
If your digestion has become something you organise your life around, never quite sure when bloating, cramping or an urgent dash to the loo will strike, you are not imagining it and you are far from alone. Irritable bowel syndrome (IBS) affects a large share of UK adults, yet most people are handed the diagnosis with little explanation of why it is happening.
That “why” matters, because IBS is not one thing. It is a pattern of symptoms that can be driven by several different underlying problems, and the support that helps depends entirely on which of those is at work in you. This guide explains what IBS really is, the root causes a functional medicine approach looks for, how testing can pinpoint yours, and the practical steps that follow.
IBS is among the most common conditions a gut clinic sees, yet it remains one of the most under-explained: a label for the symptom pattern, rarely a map of its cause.– Rome Foundation Global Epidemiology Study, Neurogastroenterology & Motility (2023)
What Is IBS (Irritable Bowel Syndrome)?
IBS is a common, long-term condition of the digestive system that causes recurring abdominal pain and changes in bowel habit, without any visible damage or disease in the gut itself. It is not a single disease but an umbrella term for a cluster of symptoms that tend to travel together. IBS is common, affecting an estimated one in ten to one in seven adults, so if you are living with it you are far from alone.
Because there is no single test that confirms it, IBS is a diagnosis of exclusion: a doctor reaches it after ruling out conditions such as coeliac disease, inflammatory bowel disease and infection, the approach set out in the UK’s NICE guidance on IBS. That process tells you what you do not have. It does not, on its own, tell you what is driving your symptoms, which is where a functional medicine approach begins.
Clinicians group IBS into subtypes based on the usual stool pattern: IBS-D (diarrhoea-predominant), IBS-C (constipation-predominant) and IBS-M (mixed). Knowing your subtype helps target both testing and support.
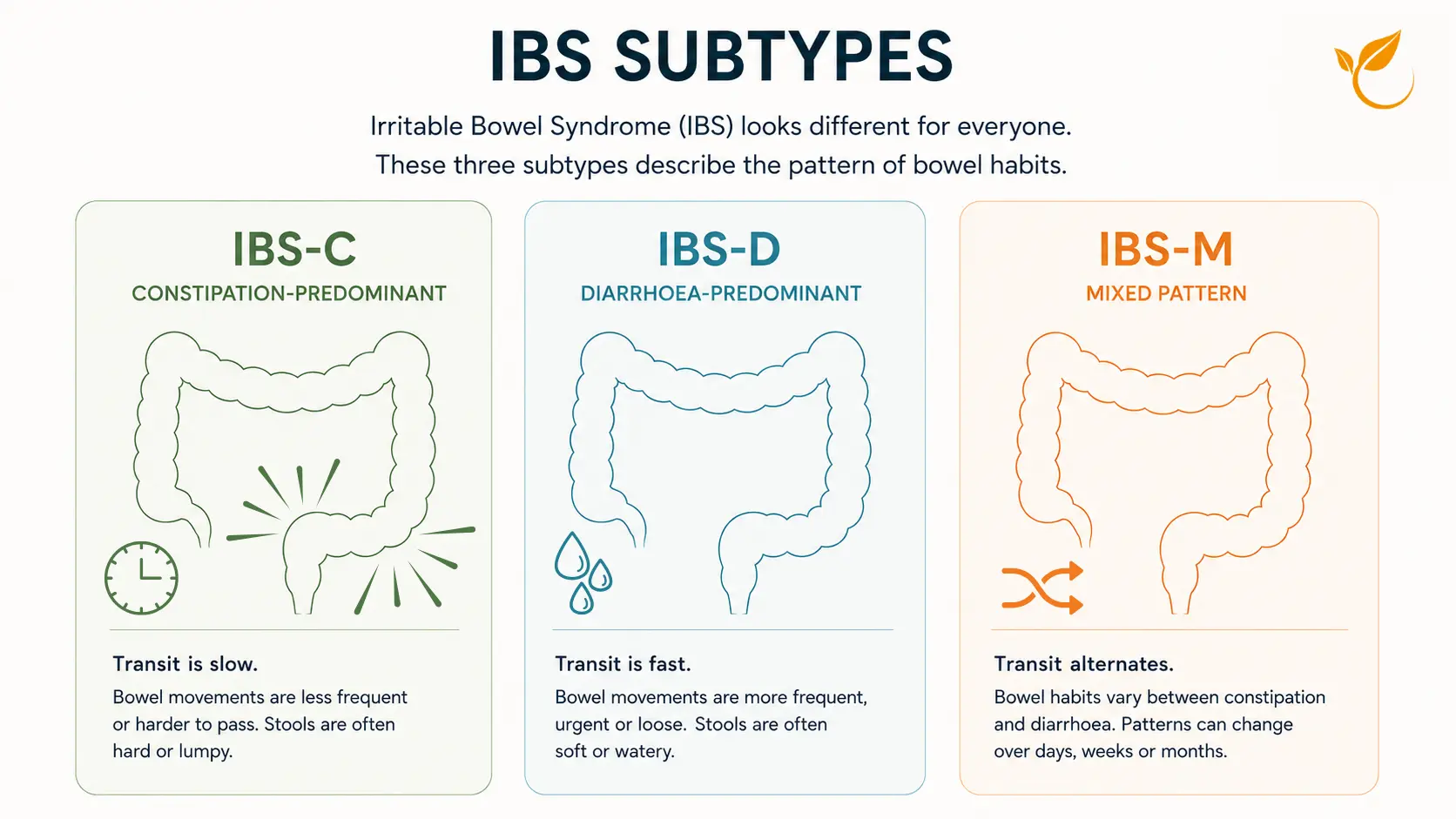
The Types of IBS: IBS-C, IBS-D and IBS-M
IBS is grouped by your usual bowel pattern, and knowing your type helps target both testing and diet:
- IBS-C (constipation-predominant): hard or infrequent stools, straining and a sense of incomplete emptying.
- IBS-D (diarrhoea-predominant): loose or frequent stools, urgency, and sometimes needing the loo soon after eating.
- IBS-M (mixed): alternating between constipation and diarrhoea.
Your subtype can change over time, so it is worth reviewing rather than assuming it is fixed.
What Are the Symptoms of IBS?
IBS symptoms vary from person to person and often flare in episodes rather than running at a constant level. The most common are:
- Abdominal pain or cramping, often eased by opening the bowels
- Bloating and visible abdominal distension
- Excess wind
- A change in bowel habit: diarrhoea, constipation, or an alternating pattern
- A feeling of incomplete emptying, or urgency
- Mucus in the stool
Symptoms are frequently worse after meals or during periods of stress, and many people notice particular foods reliably set them off.
IBS or something more serious? The red flags that need a GP
IBS does not cause bleeding or weight loss. The following are not features of IBS and should be assessed by a GP promptly: blood in the stool, unexplained weight loss, a new and persistent change in bowel habit after the age of 50, a family history of bowel or ovarian cancer, or being woken at night by pain or diarrhoea. Functional testing is not a substitute for that assessment.
What Triggers an IBS Flare-Up (and How to Calm One)?
An IBS flare-up is a spell when symptoms intensify, usually lasting a few days. Common triggers include stress, high-FODMAP or fatty foods, a change in routine, hormonal shifts and a recent gut infection.
To settle a flare, most people find it helps to eat smaller, simpler, low-trigger meals, keep hydrated, apply gentle heat to the abdomen, and use breathing or relaxation to calm the gut-brain axis. If flares are frequent or severe, that is a signal to test for the underlying driver rather than firefighting each episode.
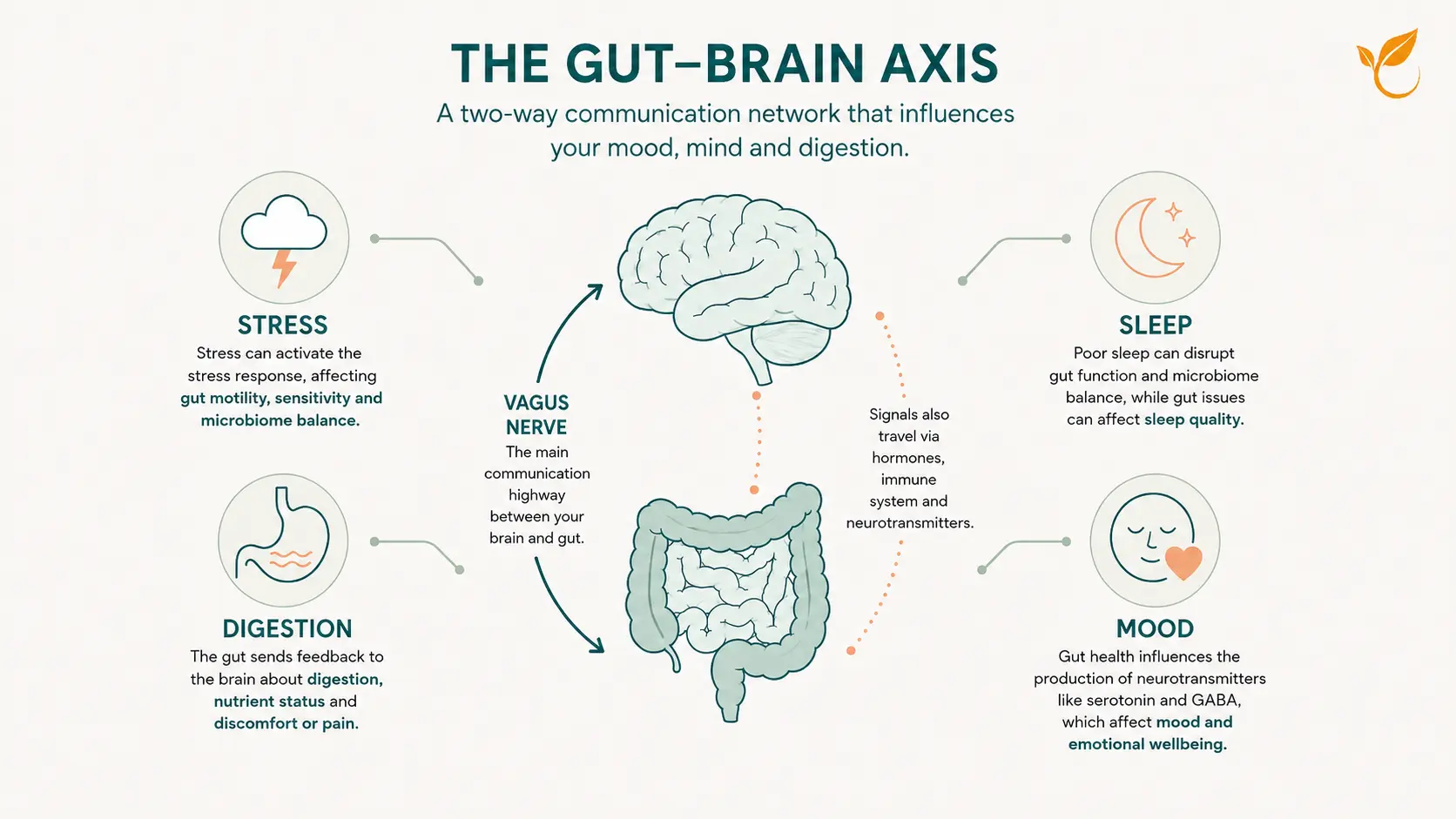
How IBS Affects the Rest of Your Body
Because the gut and brain are in constant two-way communication, IBS rarely stays confined to digestion. Many people also experience fatigue, disrupted sleep, low mood or anxiety, and a sense that their energy rises and falls with their gut. This is not a coincidence or a sign that the symptoms are imagined: the same gut-brain pathways that govern bowel function also influence mood, stress resilience and sleep.
Poorly controlled symptoms also shape daily life, from avoiding social meals to planning journeys around toilet access. Addressing the root drivers often improves more than digestion alone.
IBS in Women: Hormones, the Menstrual Cycle and Symptoms
IBS is around twice as common in women as in men, and for many the symptoms are not random: they track the menstrual cycle. Shifts in oestrogen and progesterone influence how the gut moves and how sensitive it feels, so bloating, cramping and changes in bowel habit often worsen in the days before and during a period.
This overlap is one reason IBS can be dismissed or mistaken for period symptoms. A functional medicine approach looks at the gut and the wider hormonal picture together, which is where testing helps separate what is driving what.
Does IBS Affect Men?
Yes. IBS is less common in men than in women, but it is far from rare, and it is often under-recognised because men are less likely to seek help for gut symptoms. The pattern is similar, recurring abdominal pain, bloating and a change in bowel habit, without the menstrual-cycle link. The same root-cause testing and personalised approach applies.
What Causes IBS? The Root Drivers
IBS is best understood as a disorder of gut-brain interaction. Rather than a single fault, several mechanisms can combine to produce the same symptom pattern. The drivers a functional medicine practitioner looks for include:
- Gut dysbiosis: an imbalance in the gut microbiome that alters gas production, motility and the gut lining. See our guide to gut dysbiosis.
- SIBO (small intestinal bacterial overgrowth): bacteria growing where they should not, a recognised driver of bloating and IBS-D.
- Intestinal permeability (“leaky gut”): a more porous gut lining that can drive food reactions and low-grade immune activation. More on leaky gut.
- Food intolerances and sensitivities: foods that trigger symptoms without a classic allergy, including some FODMAPs.
- Stress and the gut-brain axis: chronic stress alters motility, gut sensitivity and the microbiome.
- Digestive insufficiency: low stomach acid or enzyme output leaving food poorly broken down.
- Post-infectious IBS: symptoms that begin after a bout of gastroenteritis or food poisoning, when the gut lining and its nerves can stay over-sensitive long after the infection itself has cleared.
How to Test for IBS in the UK
There is no single test that says “this is IBS,” because IBS is diagnosed from the symptom pattern once other conditions are excluded. Functional testing does something more useful: it looks for the drivers behind your symptoms, so support can be targeted rather than generic.
The most informative starting point for most people is a comprehensive stool test. From a sample you collect at home, it maps the gut microbiome and any dysbiosis, screens for pathogens and parasites, and shows how well you are digesting and absorbing your food and whether there are markers of gut inflammation. That turns a vague sense that something is wrong into a clear, targeted picture.
Where bloating and wind dominate, or symptoms flare soon after eating, a SIBO breath test checks for bacterial overgrowth in the small intestine. Where foods clearly trigger symptoms but the culprits are unclear, a food sensitivity test helps narrow them down. The right combination depends on your subtype and your history.
If you are not sure which test applies to you, our guide to the best gut health tests for your symptoms and the complete guide to functional testing walk through the options.
| Test | Best for | Price |
|---|---|---|
| Comprehensive Stool Test (GI MAP)Recommended Starting Point | A complete picture of your gut microbiome: dysbiosis, bloating and IBS | £390 |
| Comprehensive Stool Test (GI MAP) Plus ZonulinMost Comprehensive | Everything in the GI MAP, plus leaky gut (zonulin) testing | £455 |
| SIBO Breath Test (Lactulose) | Bloating, wind and reflux that point to bacterial overgrowth | £210 |
| Food Sensitivity & Intolerance Test (200+) | Food reactions, sensitivities and unexplained flare-ups | £280 |
| Helicobacter pylori (H. pylori) Stool Test | Suspected H. pylori infection behind gut symptoms | £180 |
| All tests are clinical-grade and analysed by leading specialist laboratories that we partner with (Nordic, CNS, Genova). | ||
Not sure which test is right for you?
A free Discovery Call lets you talk it through with our functional medicine practitioner, so you can choose with confidence rather than guessing.
Test. Don’t Guess.
Get the answers you are looking for with our range of clinical-grade at-home tests.
Easy to order. Easy to use.

How to Manage IBS with Functional Medicine
A functional medicine approach does not chase symptoms in isolation. It uses testing to understand your particular drivers, then builds a personalised plan around them. The broad steps are:
- Map your root causes with testing. Identify which drivers are present using stool, breath or food-sensitivity testing rather than guessing, so the plan is built around your biology.
- Rebalance the gut microbiome. Where testing shows dysbiosis or overgrowth, use targeted nutrition and, where needed, specific antimicrobial or probiotic support to restore a healthier balance.
- Personalise your nutrition. Match your diet to your triggers. For some this means a short, structured low-FODMAP phase followed by careful reintroduction, not a permanently restrictive diet.
- Support digestion. Address low stomach acid or enzyme output where relevant, and build meal habits that give the gut the best chance to break food down properly.
- Calm the gut-brain axis. Use stress, sleep and nervous-system support to reduce the brain’s amplification of gut signals, which often lowers pain and urgency.
- Reintroduce and rebuild for the long term. Widen the diet again as symptoms settle and put habits in place to keep the gut resilient, reviewing progress rather than staying on a restrictive plan.
The detail of each step is personal to you, which is why an IBS plan works best when it starts from testing rather than guesswork. If you would like help making sense of your symptoms or choosing a test, you can book a free discovery call.
The Best Diet for IBS: Low FODMAP and Trigger Foods
There is no single IBS diet that works for everyone, because triggers are personal. The most evidence-backed starting point is the low FODMAP diet, which temporarily reduces fermentable carbohydrates that draw water into the gut and ferment to produce gas. In randomised trials, a low FODMAP diet ranked first of all the dietary and drug options tested for overall symptom improvement, and pooled analyses report a moderate-to-large reduction in abdominal pain and bloating versus a control diet. It is designed as three phases: a short elimination, a structured reintroduction to test each FODMAP group, then a personalised long-term diet built from what you learn.
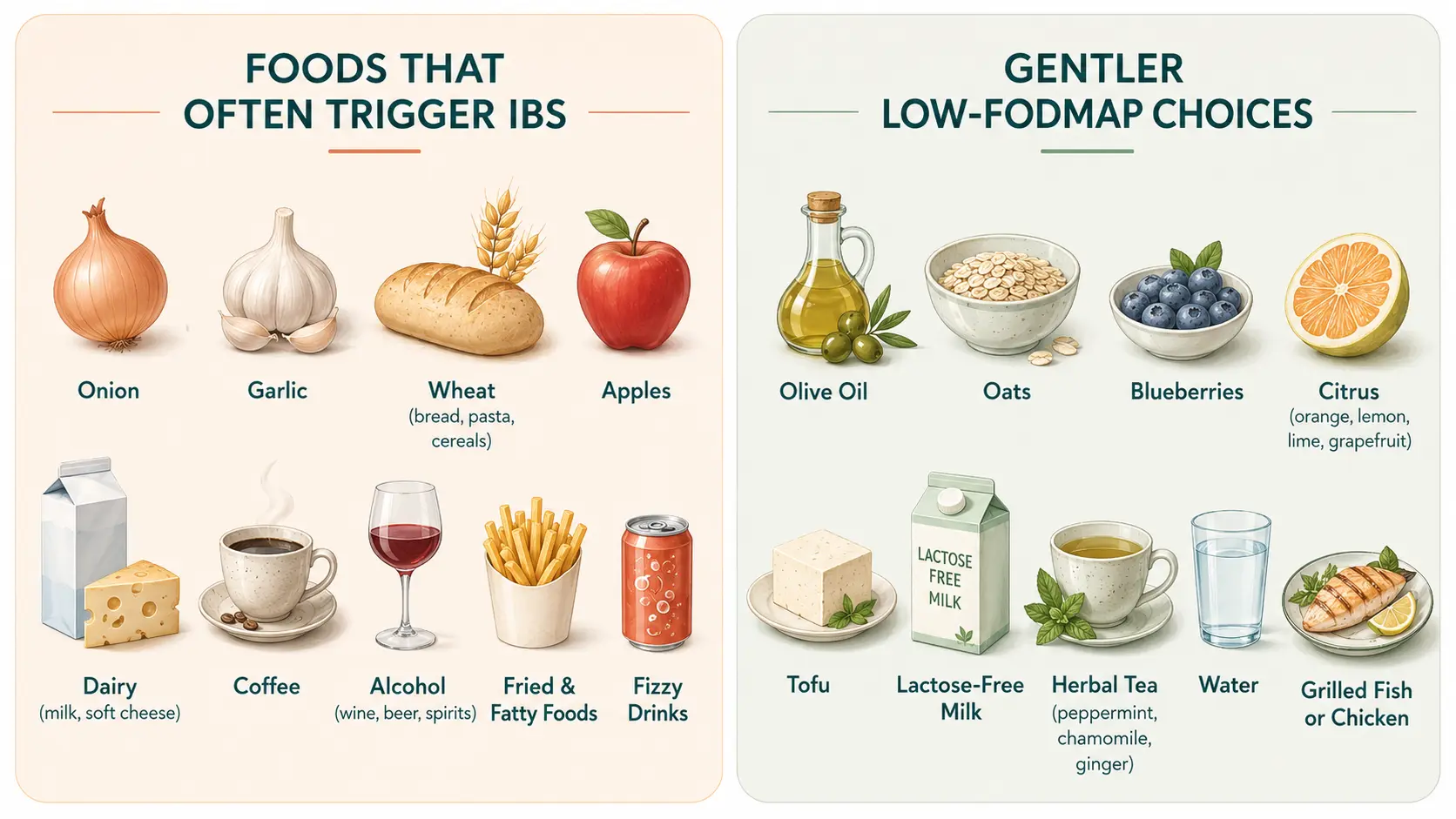
Food is one of the most common symptom triggers, so it is usually the first thing to look at. The IBS trigger foods worth reviewing first include:
- High-FODMAP foods: onion, garlic, wheat, some fruits (apple, pear, mango), pulses and certain sweeteners.
- Dairy (lactose): milk, soft cheeses and ice cream.
- Caffeine and alcohol: both can speed up or irritate the gut.
- Fatty and fried foods: frequent triggers for cramping and urgency.
- Fizzy drinks and a sudden increase in insoluble fibre: can worsen bloating and wind.
The low FODMAP diet is not meant to be permanent. It works best as a short, structured elimination of four to six weeks followed by careful reintroduction, ideally with a practitioner, so you end up with the widest possible diet rather than a needlessly restrictive one. Where food reactions are unclear, a Food Sensitivity and Intolerance Test can help pinpoint them.
Beyond FODMAPs, a few general principles help most people: favour soluble fibre such as oats and psyllium over a sudden jump in insoluble fibre, eat regular unhurried meals, and go easy on very large or very fatty meals. Because the low FODMAP approach is restrictive, it is best done with a practitioner rather than followed indefinitely, so your nutrition and gut diversity are protected.
Frequently Asked Questions About IBS
Is IBS a real medical condition?
Yes. IBS is a recognised long-term disorder of gut-brain interaction. It causes genuine symptoms even though standard tests such as endoscopy show no visible damage, which is why it is diagnosed from the symptom pattern once other conditions are excluded.
What is the difference between IBS and IBD?
IBS (irritable bowel syndrome) is a functional disorder with no visible inflammation or damage to the bowel. IBD (inflammatory bowel disease, such as Crohn’s disease or ulcerative colitis) causes measurable inflammation and tissue damage that shows on stool markers and endoscopy. Symptoms can overlap, so bleeding, weight loss or raised inflammatory markers should always be investigated.
Can a stool test diagnose IBS?
No single test diagnoses IBS, because it is a diagnosis of exclusion. A comprehensive stool test does something more useful: it looks for the drivers behind the symptoms, such as dysbiosis, pathogens, poor digestion and gut inflammation, so support can be targeted.
What is the best test for IBS in the UK?
There is no single best test for everyone. For most presentations a comprehensive stool test (GI-MAP) gives the broadest picture. A SIBO breath test is added where bloating and small-intestinal overgrowth are suspected, and a food sensitivity test helps when foods clearly trigger symptoms but the culprits are unclear.
Can food intolerances cause IBS symptoms?
Food intolerances and sensitivities can trigger or worsen IBS symptoms in many people, and fermentable carbohydrates known as FODMAPs are a common trigger. This is different from a food allergy. Identifying your triggers, sometimes with testing and a structured elimination and reintroduction, can reduce symptoms considerably.
Does stress cause IBS?
Stress does not cause IBS on its own, but it is a powerful modifier. Because the gut and brain are closely linked, stress can change gut motility, sensitivity and the microbiome, which is why symptoms so often flare during difficult periods. Managing stress is part of a complete IBS plan.
Can IBS be cured?
IBS is best thought of as something that can be managed very well rather than cured in the conventional sense. When the underlying drivers are identified and addressed, many people find their symptoms reduce substantially or settle, and learn how to keep them settled.
When should I see a doctor about IBS symptoms?
See a GP if you have any red-flag symptoms: blood in the stool, unexplained weight loss, a new and persistent change in bowel habit after 50, a family history of bowel or ovarian cancer, or being woken at night by pain or diarrhoea. These are not features of IBS and need proper assessment.
What foods should I avoid with IBS?
Common IBS trigger foods include high-FODMAP foods such as onion, garlic and wheat, dairy (lactose), caffeine, alcohol, and fatty or fried foods. Triggers are individual, so the most reliable approach is a short low-FODMAP elimination and reintroduction, or food-sensitivity testing, to find yours rather than cutting out foods unnecessarily.
How long does an IBS flare-up last?
Most IBS flare-ups build over a day or two and settle within a few days, though some last a week or more depending on the trigger and how quickly it is addressed. Frequent or long-lasting flares are a reason to test for the underlying driver.
Is IBS more common in women?
Yes. IBS is roughly twice as common in women as in men, and symptoms often track the menstrual cycle because shifts in oestrogen and progesterone affect how the gut moves and how sensitive it feels.
YOUR HEALTH. YOUR CHOICE.
Managing IBS is rarely about a single diet or one supplement. It is about finding which drivers are tipping your gut out of balance, and addressing them in the right order.
At Nutrition Diets Clinic, we identify and correct the imbalances behind your symptoms using the functional medicine approach: expert one-to-one nutritional therapy, personalised nutrition, targeted testing and lifestyle support, all built around you.